
Computer generated COVID-19 Coronavirus particle
By Christopher Sellers, Leif Fredrickson, Alissa Cordner, Kelsey Breseman, Eric Nost, Kelly Wilkins, and EDGI
Executive Summary
The administration of President Donald Trump has repeatedly undermined science-based policy as well as research that protects public health. That undermining has eroded our government’s capacity to respond to the coronavirus — from the White House itself to the labs and offices of the Centers for Disease Control (CDC), the federal government’s lead agency for science-based public health. The Trump administration’s widely-reported disbanding of the National Security Council’s directorate charged with global health has, according to many experts, hobbled the United States’ efforts against this pandemic. So have budget cuts at the CDC. Yet the U.S. would be far less prepared had Congress followed the White House’s drastic proposals to cut even more of the CDC’s budget. Moreover, we would be investing less to understand and prevent those chronic diseases that kill most Americans and that make Americans more vulnerable to the coronavirus.
Our report highlights:
- How the Trump administration has consistently sought deep cuts to the CDC’s overall budget.
- Its annual proposed cuts have ranged from just over 10 to nearly 20 percent.
- Its quest to overturn the Affordable Care Act would also have deprived the CDC of as much as 8 percent of its yearly funding.
- Though now pushing for massive federal funds to reactively fight COVID-19, the Trump administration has repeatedly (and sometimes successfully) sought to shear funding that protects us against global pandemics.
- In 2018, the Trump administration sought to reject further funding for a global health security initiative started by the CDC and USAID in response to the 2014-2015 Ebola epidemic.
- Between 2017 and 2020, the Trump administration got rid of most of CDC’s staff working on global health security in China, reducing 11 “U.S. assignees” to 3, and 39 “local employees” down to 11.
- In 2018, the administration unsuccessfully proposed turning back $252 million already appropriated to help restore health care systems in Africa still suffering from the Ebola epidemic.
- The administration has sought cuts ranging from 7 to 19 percent in the CDC’s Global Health program. That program has suffered some of the agency’s biggest staff reductions, with a loss of 72 full time staff since 2016.
- For Fiscal Year (FY) 2020, the administration proposed a 20 percent cut to the CDC’s Emerging and Zoonotic Diseases program, which is charged with investigating and preventing newly emergent diseases like the novel coronavirus.
- For infectious disease-related emergencies, the Trump administration has generally sought to shift emergency-response resources out of the more public-health oriented and science-based CDC programs to more disaster response and security-minded government niches.
- While the Assistant Secretary for Preparedness and Response (ASPR) in the Department of Health and Human Services has also seen substantial budget cuts under Trump, several ASPR programs have seen only relatively slight cuts (the Biomedical Advanced Research and Development Authority, or BARDA) or even slight increases (the National Disaster Medical System) in their proposed budgets during the Trump years.
- ASPR acquired the Strategic National Stockpile (SNS) from CDC in FY 2019. The SNS is supposed to provide a reservoir of hospital supplies and drugs for nationwide medical emergencies. Proposed cuts for the SNS annual budget over the Trump years went no higher than 5% and averaged only .5%.
- The Trump administration has generally sought more drastic cuts for programs dealing with non-infectious disease, especially for chronic ailments and environmental and occupational health.
- The administration has sought severe cuts to the CDC’s Chronic Disease Prevention and Health Promotion programs every year, with an average annual proposed cut of 21.9%. The Chronic Disease Prevention program has lost 61 full time staff since 2016.
- The administration has sought deep cuts to the CDC’s Environmental Health program every year, with an average proposed cut of 22.6%.
- Similarly, the administration has put the Agency for Toxic Substances and Disease Registry on the chopping block every year, with an average proposed cut of 17.5%.
- Targeted for the most severe budget cuts has been the National Institute for Occupational Health and Safety, with an average proposed reduction of 57%.
- The Trump administration’s handling of the CDC over the last three years reflects its general antipathy toward science:
- It has especially sought to defund programs that are heavily dependent on scientific investigation, such as those that seek to understand chronic and emerging diseases and environmental and occupational health.
- It has both proposed and implemented cuts to the CDC’s Public Health Scientific Services (PHSS), now renamed Public Health Science and Surveillance. Proposed cuts to this program have averaged 8.5% each year, and actual staff loss since 2016 is the largest of any CDC program, totaling 148 full time staff, or nearly 10% of its workforce.
- Though the Trump administration’s budgets may appear to prioritize treatment of infectious diseases while slashing chronic or other environmentally-induced disease, this distinction is not respected by COVID-19. In reality, chronic ailments make people more vulnerable to death or hospitalization from this as well as many other infectious diseases.
- While the CDC has indeed undergone an erosion of budget and staff under Trump, Congress has so far rejected most of the administration’s budget-slashing, minimalist vision for the CDC and public health. If it had not, thousands more Americans would likely die over the next few months because of even more reduced capacity at the CDC. If we cannot draw lessons here for our future, then the risks Americans face both from emerging and chronic diseases will become truly incalculable.
Un-preparing Us:
Coronavirus and The Three-Year Trump Quest to Slash Science at the CDC
The devastatingly slow and fumbling response of the Trump administration to COVID-19 has exposed not just the administration’s ineptitude, but a larger project to reduce federal capacity in public health and environmental science to a bare minimum. Largely below the radar of public awareness, the Trump administration has enrolled us all in a far-reaching and potentially fatal experiment to test how little knowledge and expertise our government can get away with. For a Centers for Disease Control and Prevention (CDC) now at the forefront of the federal push against the pandemic, the answer seems obvious: they went too far.
The Trump White House came in with the opportunity to learn from the many lessons drawn from a successful containment of the threat of Ebola in 2014-15, and could have bent more of an ear to public health professionals than to short-sighted business advocates and vilifiers of a “deep state.” Had it done either, the U.S. would be much further along the road toward controlling this epidemic. Instead, from the White House down into the labs and hallways of the CDC, the administration has pursued a minimalist and “security”-minded approach to our nation’s public health that has worsened our vulnerability to today’s COVID-19 crisis. Some of the proposed as well as actual reductions have directly targeted programs that shield us from the impacts of infectious epidemics. The Trump administration has slashed with special alacrity at this agency’s overall scientific capacity and initiatives to protect environmental health and quell chronic disease, whose sufferers are the most likely to die from coronavirus.
Researchers from the Environmental Data & Governance Initiative analyzed data on CDC budgetary proposals and staffing cuts from the CDC Budget Justifications to Congress for fiscal years 2013 to 2021. We found that the Trump administration has indeed succeeded in shearing the CDC’s capacities, undermining the federal government’s ability to respond to the crisis at hand. Comparison of actual funding and staffing trends with Trump administration proposals also shows how much worse off we would have been had it gotten more of its budget-slashing way. We have Congress to thank for why the federal scientific capacity in public health has retained the integrity it has, instead of becoming that mere shadow of itself that Trump officials have more or less intentionally sought.
Within the White House: The most obvious and well-reported loss of scientific capacity in public health has been the cuts to relevant White House staff. In mid-2018, newly arriving National Security Advisor John Bolton reorganized and “streamlined” the National Security Council (NSC) in ways that undermined its capacity to respond to pandemic threats. In April, Bolton forced out Homeland Security Advisor Tom Bossert, a strong advocate of strategic planning for pandemics. In May, Timothy Ziemer, the top White House official leading responses to pandemics, left the NSC and was not replaced. That left the NSC with no senior administrator focused solely on global health security. Moreover, the Global Health Security and Biodefense Directorate that Ziemer led was broken up, with members redistributed to other units in the NSC. At the time, many global health experts expressed concern that this move would leave the NSC flat-footed in the face of a pandemic. A White House with very few scientific advisors thereby downgraded what few avenues of information it had about emerging health threats. That loss was aggravated by Trump’s discontinuance of an Obama-appointed President Council of Advisors on Science and Technology (PCAST), which had warned in November 2016 about “the increasing emergence of naturally-occurring infectious diseases.” When Trump then belatedly reconstituted the group in October 2018, his own PCAST consisted almost entirely of business leaders, only one of whom had any direct public health experience.
The Global Health Security and Biodefense Directorate that Trump disbanded around the same time had also addressed the complex problem of managing a fragmented and territorial landscape of federal public-health expertise. As the NSC had come to recognize five years ago in the course of the Ebola epidemic, to marshal the full array of federal capabilities, the CDC has to be coordinated with a bewildering patchwork of other staff and resources all prone to intense and divisive jockeying, from Health and Human Services’s Food and Drug Administration to its Assistant Secretary of Preparedness and Response. Thanks to its 2018 dismantling of the Global Health Security and Biodefense Directorate designed precisely to overcome this problem, the Trump administration found itself without any such coordinating office in place in early 2020 as COVID-19 spread out from Wuhan and into the United States. The White House spent weeks downplaying the threat, then went through a very public musical-chairs exercise in who would lead the administration’s response. After Vice President Mike Pence took nominal charge, the struggle has continued over just which federal agencies will take which roles. Dr. Anthony Fauci, director of the infectious disease division of the National Institutes of Health and member of the White House Coronavirus Task Force, has publicly regretted the NSC global health directorate’s demise; as he put it, “we worked very well with that office.“
Inside the CDC: Thus far, the CDC, as the nation’s flagship disease-fighting agency, has stood front and center in the federal mobilization against the virus. As far as science-dependent environmental and public health federal agencies go, it has weathered the Trump era relatively well. While its appropriations (budget authority) since FY 2016 have remained nearly level in nominal dollars (Chart 1), the CDC over the Trump years has undergone a slow but corrosive decline in available resources. The yearly budget for the agency as a whole has dropped 4% between fiscal years 2016 and 2019, adjusting for inflation (Chart 1). Overall programmatic spending has fallen 6%. Similarly, overall staff at the CDC has fallen off 4.87% over those years, from 11,421 to 10,865 (in Full-Time Equivalents).
Unlike the politically-appointed leadership at other science-based agencies such as the Environmental Protection Agency, virologist Robert Redfield stepped into leadership of the CDC in March of 2018 vowing to uphold the agency’s “science-based, data-driven” approach, which he touted as helping it to protect Americans “from that which we don’t expect.” While his appointment was contested by many science and public health advocates questioning his qualifications and sometime alignment with “abstinence” solutions to the AIDS crisis, Redfield has overseen a scientific workforce that upon his arrival felt more confident in the scientific basis of their agency’s decision-making than those at others such as the Environmental Protection Agency and the Fish and Wildlife Service, according to a Union of Concerned Scientists survey.
The damage would have been far worse had Congress not stood in the way of repeated defunding attempts by the Trump administration. In its first two years, the Trump budgets proposed to slash the CDC’s appropriation by 18.2% and then by 17.1% (accounting for inflation). Today, its FY 2021 budget still seeks a cut of over 10%. Even when Republicans controlled both houses, Congress roundly rejected these aggressive Executive-led cuts, to maintain the agency’s funding near the previous year’s level.

Chart 1: Trump White House proposed budget cuts to CDC, FYs 2018-2021, compared to inflation-adjusted appropriations FYs 2013-2021. The Trump White House has consistently sought cuts of between 10 and nearly 20 percent in the CDC’s budget. Inflation adjustments in this and succeeding charts are based on 2012=$1.00. Source: [EDGI-compiled data with source links]
Nor have the administration’s efforts to slash CDC funding been confined to its annual budget requests. Overturning the Affordable Care Act (a.k.a. Obamacare) would have had dire consequences for the agency, since as much as 8% of the CDC’s yearly funding comes from transfers out of ACA funds (Chart 2). Though a close vote in a Republican Congress in July of 2017 upheld the ACA, the repeal of Obamacare remains on the White House wish list.

Chart 2: CDC Funding Sources. Just under half of the funds supporting the CDC’s activities come through Congressional authorization of its annual budget. Other support comes from a Prevention and Public Health Transfer Fund channeled from ACA allocations, as well as funds contributed by state governments to run its childhood vaccination programs. Source: [EDGI-compiled data with source links]
Global Health: Though it is now pushing for big influxes of federal funds to fight COVID-19, over the last three years the Trump administration has repeatedly sought to shear funding streams explicitly set up to protect us against global pandemics. In the wake of the 2014-15 Ebola epidemic, a global health security initiative began under auspices of the CDC and USAID and coordinated by the World Health Organization to advise and support infectious disease preparedness in corners of the world where it was most lacking. While the Ebola response was criticized for not adequately engaging with Africa’s own stricken communities, its success in mostly containing the epidemic there showed how “it is far cheaper and easier to contain infectious disease threats at the source, rather than waiting for them to reach US soil.” In 2018, the Trump administration decided not to request further funding for this program, and the CDC warned it might have to scale down this initiative from 49 countries to just 10 that seemed to present the most risks. The agency later claimed, contrary to some news reports, that Congressional appropriations enabled the continuation of many of these programs. But CDC’s China global health security staff does indeed appear to have dwindled between 2017 and 2020, from 11 “U.S. assignees” down to 3, and from 39 “local employees” down to 11 (Chart 3).

Chart 3: CDC Global Health Personnel Assigned to China. Under Trump and just prior to the COVID-19 outbreak, the CDC drastically reduced its personnel devoted to public health in China, by 70%. Source: [EDGI-compiled data with source links]
Trump efforts to reduce spending have dramatically and consistently taken aim at programs most likely to reveal and tackle potential pandemic origin points around the world. During its 2018 offensive against public health spending, the White House proposed to turn back $252 million already appropriated to restore health care systems in parts of Africa still ravaged by the earlier Ebola epidemic, just as another outbreak was beginning in the Congo. After drawing fire from both sides of the Congressional aisle, the proposal was withdrawn. The White House budget axe then took aim at funding for the CDC’s Global Health program, though proposed cuts gradually ratcheted downward from over 19% in FY 2018 to just over 7% by FY 2021 (Chart 4). The Emerging and Zoonotic Diseases program is charged with investigating and preventing new infections — like COVID-19 — and those that “have increased recently or are threatening to increase in the near future”. The Trump administration’s proposed cuts to this critical program grew over time, from just over 12% in its FY 2018 proposal (presented in 2017) to nearly 20% in FY 2020 as well as FY 2021 proposals, or nearly one-fifth of this program’s budget (Chart 5).

Chart 4: Proposed and allocated funding for CDC’s Global Health Program (inflation adjusted). Source: [EDGI-compiled data with source links]

Chart 5: Proposed and allocated funding for CDC’s Emerging and Zoonotic Diseases Program (inflation adjusted). Source: [EDGI-compiled data with source links]
Public Health Preparedness and Response: Though very few CDC programs have been spared by the Trump White House’s prospective budgetary axe, for some the blows have been more glancing. The Public Health Preparedness and Response supports the development of standards for how state, local, and tribal governments might best prepare for emergencies. The Trump White House initially sought to cut funding to this program by over 16% (Chart 6) but then dialed down its proposed cuts, mostly recently to only 3% for FY 2021. Programs that provide assistance once epidemics are already upon us have not been spared, though they have seen more modest proposed reductions. For example, the Strategic National Stockpile (SNS) provides a reservoir for hospital supplies — from masks, drugs, and disinfectants to respirators — mainly for clinical treatment of those who become sick. While its proposed FY 2019 budget was almost 5% lower, annual cuts during the Trump Presidency have averaged about .5% (Chart 7).
Starting in FY 2019, the SNS was switched out of the CDC into the hands of the Health and Human Services’ Assistant Secretary for Preparedness and Response (ASPR). The stated goal was to make more efficient use of the stockpile across a wider range of disasters: to “optimiz[e] MCM [medical countermeasure] development, response, and utilization” in the face of “chemical, biological, radiological, or nuclear (CBRN) threats or emerging infectious diseases,” as well extreme weather. At the time, the American Public Health Association raised serious questions about the wisdom of the transfer, and in retrospect, it is easy to see how movement of a $500+ million program from one agency to another could pose immense bureaucratic challenges, hobbling its operations and efficiency for years to come. Trump’s recent admonishment of state officials to “try getting [ventilators] yourselves” may well reflect the ASPR’s inability to “optimize” stockpile operations in time, leaving hospitals in the lurch just as they prepare to treat the anticipated hundreds of thousands of COVID-19 patients.
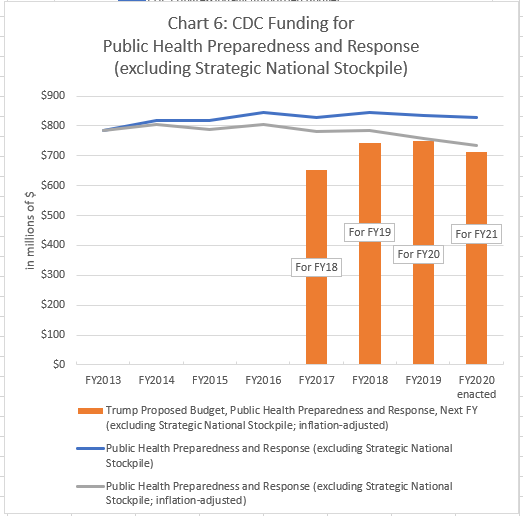
Chart 6: Proposed and allocated funding for CDC’s Public Health Preparedness and Response program (inflation adjusted). Source: [EDGI-compiled data with source links]

Chart 7: Proposed and allocated funding for the Strategic National Stockpile, transferred to ATSDR in 2019 (inflation adjusted). Source: [EDGI-compiled data with source links]
From Preventative toward Reactive Public Health: HHS’s Assistant Secretary for Preparedness and Response: The transfer of the SNS points to a larger pattern: the Trump administration is gradually shifting emergency-response resources out from the more public-health oriented and science-based CDC into more disaster- and security-minded governmental niches that developed in the early 2000s in the wake of 9-11 and Hurricane Katrina. The ASPR, itself a product of this era, grew during the Obama Administration and has been among those federal public health agencies targeted by the budget proposals of the Trump White House, with annual proposed cuts averaging 6.46%, including a 14.64% slash for FY 2019 (Chart 8). White House budget proposals for ASPR’s Hospital Preparedness program have remained in the red, averaging a 5.9% decrease. Nevertheless, consolidation of resources like the SNS into the ASPR has appealed to an administration generally eager to appease the private sector, for instance, through deregulation. The ASPR’s Biomedical Research and Development Authority (BARDA) works with pharmaceutical and other medical suppliers to develop and enable the distribution (and sales) of medical responses — in this moment, a vaccine for COVID-19. BARDA’s proposed budget cuts over the Trump years have averaged only 1.1% nd White House budget proposals for ASPR’s National Disaster Medical System have actually stayed in the black, with budgetary boosts over the two years bringing its average gains to 18.9% per year.

Chart 8: Funding of the Assistant Secretary for Preparedness and Response (ASPR) in the Department of Health and Human Services. This governmental unit now oversees the Strategic National Stockpile. It also includes the Biomedical Research and Development Authority, currently seeking a vaccine for COVID-19, as well as the National Disaster Medical System. Source: [EDGI-compiled data with source links]
Though the Trump administration has sought to cut public health funding across the board, the skewed severity of cuts shows a clear favoring of a reactive rather than a preventative public health strategy. Trump’s proposed cuts have been lighter in areas of public health dealing with infectious disease, especially responding to threats that have already made people sick or have already arrived on our shores. However, parts of the CDC that are more prevention-minded have been the target of the most severe cuts in Trump budget proposals. The most targeted programs deal, by and large, with diseases that are not infectious at all, but are longer-acting both in their causes and in their consequences — that is, chronic diseases like cancer or diabetes.
The Continuing Importance of Chronic Disease: The shift from a preventative toward a reactive strategy, reinforced by the growing emphasis on health “security,” is re-orienting federal public health away from where it should be focused: on positive health outcomes. As a March 16 CDC briefing shows, COVID-19 has the highest mortality among people with serious underlying health conditions. Here, COVID-19 is hardly alone; many infectious diseases are more dangerous for those afflicted with debilitating chronic ailments like diabetes or cancer. Addressing these underlying vulnerabilities adds much to the protection of large populations from infectious epidemics, in addition to bringing down mortality from diseases that kill millions of Americans each year. Moreover preventative public health as well as healthcare, often working through what we have come to understand as risk factors for chronic disease in our workplaces and larger environments, is more effective and cheaper than healthcare that people require after they become sick. By seeking to reduce funding to programs critical to preventative public health, the Trump administration has laid the groundwork for bolstering both the scope and the magnitude of the crisis we now face.
Compared to the prevention of infectious diseases, the prevention of chronic disease is harder to square with the “health security” and bioterrorism-oriented public health that the White House seems to favor. Consequently, cuts for the Chronic Disease Prevention and Health Promotion program have been among the most severe and consistently proposed (Chart 9).

Chart 9: Proposed and allocated funding for CDC’s Chronic Disease Prevention and Health Promotion program (inflation adjusted). Source: [EDGI-compiled data with source links]
Downsizing Science: The defunding of research on both chronic and emerging diseases is consistent with the Trump administration’s broader disregard for science. Emerging diseases frequently pose medical mysteries through their novelty and prevention of chronic diseases have long and complex causal chains to unpack. Both demand considerable investments in scientific study. The White House’s ongoing vision for downsizing chronic disease prevention at the CDC thereby conforms to a theme that many other parts of the federal government have come to know: its disregard for and defunding of science.
In response to a Trump Executive Order, the CDC, one of the most science-dependent federal agencies, has quietly set about disbanding scientific advisory committees, starting with, among others, a Board of Scientific Counselors for its National Center for Environmental Health and Agency for Toxic Substances and Disease Registry. The CDC’s Public Health Scientific Services, now renamed “Public Health Science and Surveillance,” has been repeatedly targeted for budget reductions as high as 11%, averaging 8.5% during the Trump years (Chart 10). Charged with “set[ting] and promot[ing] agencywide scientific priorities,” as well as with disease surveillance and the gathering of statistics on Americans’ health, the division has borne the brunt not just of proposed budget cuts but of actual reductions in staff (Charts 11 and 12). From FY 2016, the Public Health Scientific Services Division experienced the highest volume of staffing cuts of any major CDC unit. It lost 148 staff Full Time Equivalents (FTEs), or nearly 10% of the workforce, followed by staffing for Global Health, which lost 72 staff, and Chronic Diseases, which lost 61 FTEs.

Chart 10: Proposed and allocated funding for CDC’s Public Health Scientific Services program (inflation adjusted). Source: [EDGI-compiled data with source links]

Chart 11: Percent Change in Full-Time Equivalent Staff Across CDC’s Major Divisions, FY 2016-FY 2019. Source: [EDGI-compiled data with source links]

Chart 12: Numerical Change in Full-Time Equivalent Staff Across CDC’s Major Divisions, FY 2016-FY 2019. Source: [EDGI-compiled data with source links]
Neglecting Environmental and Occupational Health: Not only does the public health understanding and prevention of chronic disease often hinge on extensive scientific inquiry, compared to that of infectious disease it is also not as easily or readily confined to medical facilities and pharmaceutical treatments. Instead, it can point toward needed interventions in people’s environments, and by extension, in corporate behavior. By illuminating the impacts of toxic pollutants or workplaces on health outcomes, public health research can implicate business communities — communities that the Trump administration has shown itself eager to please and placate.
For instance, the Environmental Health Division of the CDC includes programs on childhood lead poisoning, implicating landlords of rental housing, on air quality, threatened by local industries, as well as an initiative on climate change and health. The ATSDR funds studies of industrial contaminants from arsenic to PFAS, and provides authoritative publicly accessible portals for existing knowledge about toxic chemicals. Not surprisingly, then, those parts of the CDC that deal with environmental health, as well as the closely connected ATSDR, have been targeted with some of the biggest chops from the Trump budget axe (Charts 13 and 14). Compared to proposed cuts for the CDC overall, ranging from 10-18% and averaging 14.7%, those for ATSDR averaged 17.5% and those for Environmental Health Division peaked with a 27% cut for FY 2018 but averaged 22.6% over the Trump years.

Chart 13: Proposed and allocated funding for CDC’s Environmental Health Division (inflation adjusted). Source:[EDGI-compiled data with source links]

Chart 14: Proposed and allocated funding for the Agency for Toxic Substances and Disease Registry (inflation adjusted). Source:[EDGI-compiled data with source links]
As the Trump Office of Management and Budget (OMB) claims, while its most recent cuts to CDC more effectively prioritize “programs that focus on infectious disease and emergency preparedness activities,” it fully acknowledges it is slashing funds for “non-infectious activities.” Yet the OMB’s report plucks out a single example it would have us take as illustrative of unnecessary health research: “studying the health and safety risks of infrequent bathroom breaks for taxi drivers.” With this example, the Trump White House demonstrates its contempt not just for chronic-disease and environmental health research per se, but especially, for any scientific study of workers’ health risks.
Indeed, no part of the CDC has been more harshly treated by the Trump OMB than the National Institute for Occupational Safety and Health (NIOSH), the agency which researches occupational illness and injury under the CDC umbrella (Chart 15). The White House’s FY 2018, 2020, and 2021 budget proposals included cuts of at least 40% to NIOSH, while the FY 2019 proposal called for the agency’s complete elimination. Zeroing out this budget line would have essentially abolished what has long been a bulwark institution for protecting the health of American workers.

Chart 15: Proposed and allocated funding for CDC’s National Institute for Occupational Safety and Health program (inflation adjusted). Source: [EDGI-compiled data with source links]
Conclusion: If the Trump administration had had its way, our powers to act against COVID-19, limited as they now are, would have been utterly crippled. Trump White House budgeting has relentlessly sought to downsize the CDC. Though Congress has stood in the way of the worst of its intentions, this administration has still been able to eliminate a host of staff that would have better shielded Americans from the current pandemic, from the NSC’s global health security directorate to the CDC’s global health team for China, which was shrunken by two-thirds just in time for the coronavirus’s onslaught. Deliberately and successfully, the Trump White House has impaired the federal government’s capacities to respond, as confirmed in October 2019 by a simulation run by Trump’s very own Health and Human Services Department. It showed “just how underfunded, underprepared and uncoordinated the federal government would be for a life-or-death battle with a virus for which no treatment existed.” Even then, little more was done to strengthen our ability to respond to precisely the public health disaster we now face.
While the public health of infectious diseases seems of overriding importance in the midst of a pandemic such as this one, the Trump administration’s even more destructive designs for the public health of non-infectious diseases also have relevance to our efforts against the novel coronavirus. Programs involving disease prevention, chronic illnesses, and environmental and occupational health, hit the hardest by the White House’s budget proposals, can alleviate those underlying chronic health conditions that make so many Americans more vulnerable to the ravages of COVID-19.
The Trump administration’s budgets also reveal an ongoing shift of federal resources for combating infectious disease from a science-centered and prevention-minded agency like the CDC into agencies with more reactive and “security”-minded perspectives, like HSS’s Assistant Secretary for Preparedness and Response. In public health, as in so many other realms of federal activity, scientifically-informed protections of American citizens are shriveling away, as budget and staff cuts join policy changes and rewritten rules in curbing the role of science in official decision-making. As a result, U.S. residents are having many more health threats and risks quietly foisted upon them, for a future stretching out far beyond the current pandemic.
What little protection we have experienced thus far from this harsh and dismissive vision for our nation’s landmark public health agency has, perhaps surprisingly, come from that most maligned branch of our federal government: Congress. With little publicity, not just Democrats but a contingent of Republicans have quietly acted to preserve a CDC that, hopefully, is still capable of curbing the current pandemic. Let us hope, as well, that the death-dealing consequences of shortchanging a scientifically informed and capacious public health are now being made crystal clear, and that in the coming months and years, those lessons will prevail.
For press inquiries contact edgi.comms@gmail.com